

Polycythemia - newborn
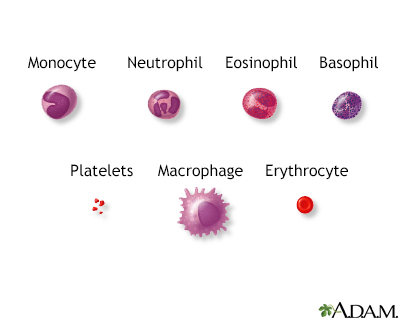
Polycythemia means there are too many red blood cells (RBCs) in an infant's blood.
Causes
The percentage of RBCs in the infant's blood is called the "hematocrit." When this is greater than 65%, polycythemia is present.
Polycythemia can result from conditions that develop before birth. These may include:
- Delay in clamping the umbilical cord
- Diabetes in the baby's birth mother
- Inherited diseases and genetic problems
- Too little oxygen reaching body tissues (hypoxia), such as from congenital heart or vascular (blood vessel) abnormalities
Congenital heart
Congenital heart disease (CHD) is a problem with the heart's structure and function that is present at birth.
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - Twin-twin transfusion syndrome (occurs when blood moves from one twin to the other)
Twin-twin transfusion syndrome
Twin-to-twin transfusion syndrome is a rare condition that occurs only in identical twins while they are in the womb.
Read Article Now Book Mark Article
The extra RBCs can slow or block the flow of blood in the smallest blood vessels. This is called hyperviscosity. This may lead to tissue death from lack of oxygen. This blocked blood flow can affect all organs, including the kidneys, lungs, and brain.
Symptoms
Symptoms may include:
- Extreme sleepiness
- Feeding problems
- Seizures
Seizures
A seizure is the physical changes in behavior that occurs during an episode of specific types of abnormal electrical activity in the brain. The term ...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article
Exams and Tests
There may be signs of breathing problems, kidney failure, low blood sugar, or newborn jaundice.
Newborn jaundice
Newborn jaundice occurs when a baby has a high level of bilirubin in the blood. Bilirubin is a yellow substance that the body creates when it replac...

If the baby has symptoms of hyperviscosity, a blood test to count the number of RBCs will be done. This test is called a hematocrit.
Other tests may include:
- Blood gases to check the oxygen level in the blood
- Blood sugar (glucose) to check for low blood sugar
- Blood urea nitrogen (BUN), a substance that forms when protein breaks down
- Serum creatinine
- Urinalysis
- Serum bilirubin
Treatment
The baby will be monitored for complications of hyperviscosity. Fluids may be given through the vein. A partial volume exchange transfusion is sometimes still done in some cases. However, there is little evidence that this is effective. It is most important to treat the underlying cause of the polycythemia.
Outlook (Prognosis)
The outlook is good for infants with mild hyperviscosity. Good results are also possible in infants who receive treatment for severe hyperviscosity. The outlook will depend largely on the reason for the condition.
Some children may have mild developmental changes. Parents should contact their health care provider if they think their child shows signs of delayed development.
Possible Complications
Complications may include:
- Death of intestinal tissue (necrotizing enterocolitis)
Death of intestinal tissue
Necrotizing enterocolitis (NEC) is the death of tissue in the intestine. It occurs most often in premature or sick babies.
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - Decreased fine motor control
- Kidney failure
- Seizures
- Stroke
Reviewed By
Neil K. Kaneshiro, MD, MHA, Clinical Professor of Pediatrics, University of Washington School of Medicine, Seattle, WA. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team.
Owusu-Ansah A, Letterio J, Ahuja SP. Red blood cell disorders in the fetus and neonate. In: Martin RJ, Fanaroff AA, eds. Fanaroff and Martin's Neonatal-Perinatal Medicine. 12th ed. Philadelphia, PA: Elsevier; 2025:chap 81.
Tashi T, Prchal JT. Primary and secondary erythrocytosis. In: Fish JD, Lipton JM, Lanzkowsky P, eds. Lanzkowsky's Manual of Pediatric Hematology and Oncology. 7th ed. Cambridge, MA: Elsevier Academic Press; 2022:chap 10.
Thom CS, Lambert MP. Blood disorders. In: Kliegman RM, St. Geme JW, Blum NJ, et al, eds. Nelson Textbook of Pediatrics. 22nd ed. Philadelphia, PA: Elsevier; 2025:chap 138.
Disclaimer
© 1997- A.D.A.M., a business unit of Ebix, Inc. Any duplication or distribution of the information contained herein is strictly prohibited.